
Facts
To understand the arguments pro and con below, here are a few preliminary facts about physician-assisted death (also often known as physician-assisted suicide by opponents and medical aid in dying by supporters) in the United States:
-
Physician-assisted death (PAD) allows eligible patients to obtain lethal medication to end their own life. In U.S. states where it is legal, PAD applies to mentally capable adults diagnosed with a terminal illness expected to cause death within six months. Laws also include procedural requirements intended to reduce the risk of impulsive, uninformed, or coerced decisions.1
-
Medical professionals evaluate eligibility and prescribe the lethal medication but do not administer it. Typically, at least two clinicians must confirm that the patient meets the legal criteria and is making an informed, voluntary decision. The lethal medication is prescribed in advance, and the patient decides whether and when to take it. The medication typically renders the patient unconscious and then stops their breathing.2
-
PAD is legal in a minority of U.S. states. PAD is authorized in 13 states and Washington, DC, though the legal basis varies: most have statutes authorizing it, while Montana allows it under a state court ruling.3 In most other states, assisting suicide is prohibited by statute, common law, or another legal provision.4
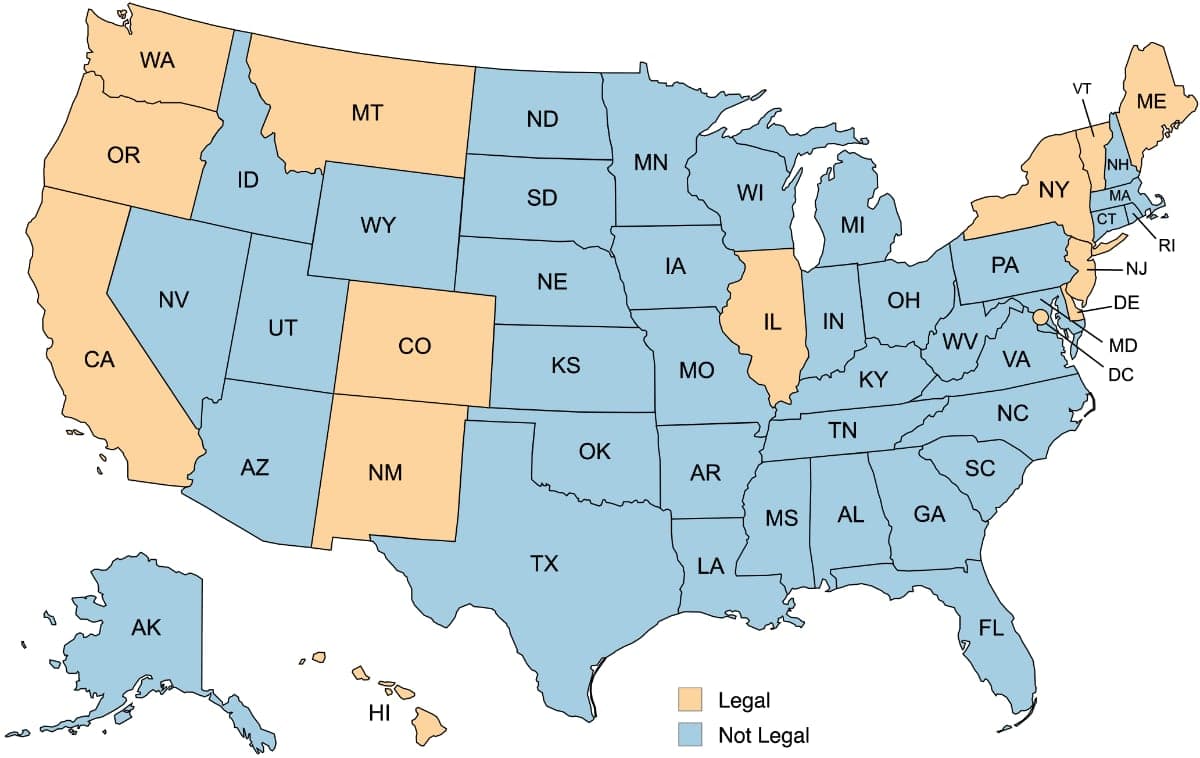
Source: Fairmind / MapChart (map), Death with Dignity (data)5
-
State laws are largely based on an Oregon law that went into effect in 1997.6 Because Oregon is the longest-running PAD state, and the model for others, we reference it throughout this guide.
-
Where it is legal, PAD accounts for a small share of deaths. In Oregon, roughly 1% of total deaths were due to PAD in 2025.7 If we only consider deaths involving terminal illness, the percentage is marginally higher but still a small number.8
-
In the United States, PAD is not euthanasia. All U.S. states require the patient to self-administer the lethal medication. In contrast, euthanasia involves a medical professional administering the lethal medication that ends the patient’s life. That said, many of the arguments for and against PAD also apply to euthanasia.
-
PAD is different from palliative care and withdrawal of treatment, which are not themselves ethically contested:
-
Palliative care manages symptoms and provides psychological support to relieve suffering. If medication used to relieve suffering hastens death, this is seen as a side effect, not the intention.
-
Honoring a patient’s request to withdraw treatment may hasten death but is seen as allowing the illness to run its course. Part of the PAD debate is whether PAD is a straightforward extension of treatment withdrawal or whether it crosses an additional and problematic moral line.
-
Factors to Consider
Below are six factors to consider about physician-assisted death, each with opposing arguments.
The debate is explained in terms of United States PAD laws as they exist today. Those laws’ requirements—terminal illness, a six-month prognosis, patient self-administration—shape the debate differently than if the guide were about more expansive PAD laws in other countries like Canada or the Netherlands. As a result, why U.S. laws draw the line where they do, and whether they will hold there, are themselves part of the debate. We address this in the Slippery Slope factor and in the Naming and Framing section of the Editorial Choices appendix. The appendix also explains other choices about language, framing, and arguments not included in the main content.
1. Mercy
The PAD debate arises from end-of-life situations where continued life may involve profound suffering—whether from physical pain, the loss of bodily function and independence, or the prospect of dying in ways the patient finds intolerable. This raises a difficult question about what mercy requires.
PAD supporters believe mercy requires giving terminally ill patients the option to end their own lives. They cite cases such as Barbara Goodfriend, who at age 83 was diagnosed with a terminal disease that would progressively erode her ability to control her own muscles. After it affected her ability to walk, she asked “What am I going to give this up for? To be in a wheelchair? To have a feeding tube? I wish I had more time to live, but I don’t want more time as a patient.” She died at home with friends and family, after having self-administered the lethal medication.9 PAD supporters call this “death with dignity” because it allows the patient to end life on their own terms. They add that one-third of patients get the prescription but don’t use it because having the option at-hand is itself a comfort.10
PAD opponents believe that mercy means caring for patients as their lives reach a natural end, not actively helping them terminate their lives. They note that today’s palliative care can meaningfully reduce physical suffering and provide psychological and emotional support at the end of life.11 Some opponents acknowledge rare cases where patients may reasonably want PAD, but they argue that tailoring policy to those exceptional cases would impose unacceptable moral and practical risks—including devaluing human life, stigmatizing disability, undermining the physician’s role as healer, and approving requests that reflect coercion or addressable despair rather than genuine choice. (We will cover these in greater detail below.)
The key question: Can PAD be an act of mercy, and if so, does legalizing it remain merciful once the wider consequences are considered?
2. Autonomy
In the PAD debate, autonomy refers to a patient’s right to make decisions about their own body and medical care. In law and standard medical practice, this means patients have the right to accept or refuse treatment, including to refuse life-sustaining treatment. However, it’s contested whether this right should extend to requesting that a physician actively and intentionally bring about death.
PAD supporters argue that PAD is a straightforward extension of the right to refuse treatment. In their view, the ethically primary question is who decides, not whether the physician is being asked to “let die” or to “actively bring about death.” They note that this distinction is already blurry in scenarios like honoring a patient’s request to be taken off a ventilator, where a physician performs an action that foreseeably and immediately brings about the patient’s death. Since such practices are widely accepted, they argue that it is difficult to identify a clear, principled basis for treating PAD differently.
PAD opponents argue that patient autonomy, while important, has accepted limits. In medicine, patients may refuse treatment, but they may not demand any intervention they choose, especially if it conflicts with core medical or social norms. In this view, PAD is not simply another exercise of autonomy but a step beyond it, because it asks the physician to prescribe lethal medication with the intent of bringing about the patient's death. Opponents say this is different from complying with a patient’s request to remove a ventilator, which only requires the physician to “let die.” They say that the step from letting die to intending to cause death is where autonomy can no longer carry the argument.
The key question: Is PAD a straightforward extension of patients’ autonomy to discontinue treatment, or a different kind of act that requires separate justification?
3. Social Effects
The PAD debate is not only about individual patients; it also concerns how legalizing PAD affects society as a whole. Some concerns focus on measurable effects, such as whether vulnerable groups will be pressured into choosing PAD. Others are about the broader message the law may send, such as whether some lives are seen as less worth living or whether patients may feel an expectation to choose PAD.
PAD supporters point to U.S. states’ experience with PAD as evidence that social concerns are largely unfounded. Oregon data show no evidence that vulnerable groups (such as low-income people, racial minorities, or women) have been disproportionately pressured into choosing PAD.12 They also note that the top concerns of Oregon PAD patients were personal, not social: loss of autonomy and the inability to do things that made life meaningful (both cited by 89% of patients).13 Supporters argue this indicates that social effects are small and safeguards work. Supporters also reject that any of this amounts to signaling that some lives are worth more than others. Rather, they see legalized PAD as affirming individuals’ rights to assess their own situations by their own values. In a society with deep disagreement about end-of-life choices, they argue, allowing that choice is the most appropriate response.
PAD opponents argue that legalizing PAD erodes a foundational cultural commitment: that every life deserves equal protection, regardless of condition. Once PAD is available, they contend, that commitment quietly gives way to the idea that some deaths are acceptable, even appropriate. Disability-rights advocates make this point most forcefully, arguing that PAD sends a message that lives marked by illness or dependence are less worth living.14 Related but distinct, opponents warn that the mere availability of PAD creates a background expectation that some patients should choose it—to avoid burdening family members or consuming scarce medical resources. They note that 40% of Oregon PAD patients cited “burden on family, friends/caregivers” as a concern related to their choosing PAD.15 For opponents, PAD represents a troubling bargain: It favors the relatively few who may genuinely want and need it, but penalizes the far larger population who don’t want PAD and whose lives are implicitly devalued by its availability, as well as those who, if vulnerable to depression or coercion, may make an irreversible choice that doesn’t reflect their authentic wishes.
The key question: Are PAD’s social costs significant enough to justify overriding the normal principle of individual choice?
4. Physicians’ Role
Although much of the PAD debate rightly centers on the patient, the involvement of the physician raises its own questions.
PAD supporters say that conventional healing is not possible at the end of terminal illness, so the physician’s imperative must be to relieve suffering. In cases where an informed patient freely decides there is no better option to relieve end-of-life suffering, they argue that PAD should be available—and that withholding it is a failure of care. They note that physicians who do not want to be involved with PAD can opt out, enabling others who see PAD as valuable to provide it. They observe that historically many physicians have quietly honored dying patients’ wishes by administering drugs like morphine in doses intended to be fatal.16 They argue that PAD helps physicians in that position by providing a process with safeguards and leaving the final action to the patient.
PAD opponents often cite the American Medical Association, which says PAD “is fundamentally incompatible with the physician’s role as healer.”17 They argue that PAD shifts physicians into roles they are not primarily trained for, such as judging whether a patient’s request is fully voluntary or distinguishing genuine end-of-life readiness from treatable depression. Although they can enlist specialists, the primary physician is still responsible. This extends to the six-month prognosis, which is normally an uncertain estimate but under PAD becomes a trigger for a potentially irreversible action—a concern given that some patients end up stabilizing and living longer.18 Although a physician could avoid these burdens by opting-out of the process, that could mean refusing a patient in their greatest time of need. In opponents’ view, the core issue with PAD is that it places physicians in this conflicted position in the first place.
What else to know: Some medical organizations, such as the American Academy of Family Physicians, have taken a neutral stance on PAD. But the largest organizations remain opposed, including the American Medical Association (AMA) and the American College of Physicians. Even so, these organizations have not sanctioned members who engage in PAD. The AMA’s Code of Ethics holds that physicians who, “after due moral consideration,” participate in PAD have not violated the Code.19
The key question: Should PAD be a legitimate medical option, or does offering it change medicine in ways we shouldn’t accept?
5. Reliability of the Patient’s Decision
All sides agree that when a patient requests PAD, the decision may not be voluntary or fully considered. Concerns focus on two main risks:
-
Undue influence from others, such as family members or caregivers who would prefer the patient die earlier. Roughly one in ten U.S. adults 60 years or older experience some form of mistreatment each year, so the risk is real.20
-
Impaired decision-making due to treatable depression. The key is to avoid despair-driven decisions that could change with treatment, support, and reflection.
The disagreement is about whether these risks should be viewed differently for PAD than treatment withdrawal, and whether PAD-specific safeguards are adequate.
PAD supporters note that every state accepts these same risks for terminal patients who decide to withdraw treatment. In comparison, they say PAD has far more safeguards and thus represents less risk. Further, supporters argue that PAD’s safeguards work. They note that since 1997, Oregon has had thousands of assisted deaths, and no case of abuse has ever been legally substantiated. Supporters acknowledge that the safeguards rely on physicians’ judgment and self-reporting, largely for privacy reasons. But they say that’s why at least two different physicians must evaluate the patient and approve the request. They argue that this provides enough ethical and legal accountability to prevent bad-faith actions and to minimize clinical error.21
PAD opponents argue that treatment withdrawal is not the same as state-sanctioned, physician-prescribed “treatment” intended to cause death. As a result, they say, societal acceptance of risks associated with treatment withdrawal does not imply the same for PAD. And in response to the idea that PAD’s safeguards address the risks, PAD opponents often cite the case of 85-year-old Kate Cheney, whose family took her to multiple physicians until her PAD request was approved, despite earlier findings of impaired judgment and concerns about a “somewhat coercive” daughter.22 They note that this case only came to light because a local newspaper discovered it independently. They argue it illustrates the lack of effectiveness and accountability of Oregon’s system, which relies on physicians’ own self-reporting, has no audit mechanism, and has physician-referred psychiatric evaluations in only a tiny fraction of cases.23
The key question: Do PAD safeguards reasonably ensure that patients’ decisions are both voluntary and sound, or are the risks too hard to detect or manage?
6. Slippery Slope
In some other countries, PAD laws have broader eligibility than current U.S. state laws. For example, Canada and the Netherlands have laws that allow PAD not just for terminal illness but also some non-terminal conditions. Both countries also allow PAD via self-administration and euthanasia. This raises the question whether U.S. laws might be subject to a “slippery slope,” where over time they expand to cover non-terminal conditions and allow euthanasia.
U.S. laws have so far retained the requirements of terminal illness (with a six-month prognosis), self-administration, and safeguards similar to Oregon’s. Since 2019, however, multiple U.S. jurisdictions have amended their laws, such as by shortening or waiving waiting periods, removing residency requirements, and authorizing nurse practitioners and physician assistants to evaluate and prescribe.24
PAD supporters argue that dire predictions of a slippery slope—to euthanasia, a “duty to die,” or other grim outcomes—have not materialized in the United States. They point to decades of experience with PAD laws in Oregon and other states, where the practice remains rare and restricted to terminally ill cases and to self-administration. Regarding some states’ amending their laws, such as to shorten waiting periods, supporters argue these are refinements in response to observed issues such as patients dying during multi-week waiting periods. More broadly, they contend that drawing and maintaining boundaries is a normal feature of law—even in morally sensitive areas—and that the key limits of U.S. PAD laws have remained stable over time.
PAD opponents argue that once you accept the principle that physicians may help patients die to relieve suffering, it becomes increasingly difficult to defend specific restrictions. If suffering justifies PAD for the terminally ill, opponents ask, why not for patients with chronic but non-terminal conditions who suffer just as much? Why require self-administration if a patient is too physically impaired to do so—isn’t that cruel? Opponents argue these aren’t hypothetical questions, pointing to Canada, where assisted-dying laws initially focused on end-of-life cases but later expanded to allow non-terminal conditions.25 They argue that what supporters see as “refinements”—changes to waiting periods, dropping residency requirements—are actually the first steps down the slippery slope.26
The key question: Should we view U.S. PAD laws’ current limits as largely fixed, or as destined to expand over time?
Example Viewpoints
The questions above represent genuine tensions without easy answers. Below are examples of how different people might weigh these and other considerations to arrive at coherent positions. You might find yourself aligning with one of these viewpoints, or you might form your own opinion by combining elements from more than one.
It’s My Life
I support the legal availability of physician-assisted death because decisions about my own body and life ultimately belong to me, not the state. If I make an informed and voluntary request for medical assistance to die, it should be honored—and the law should reflect that. Concerns about medical ethics or broader social effects matter, but they should not override my basic right to choose how I die at the end of a terminal illness. Even if others find my choice troubling, I believe the freedom to make it must remain with me.
In Practice, It Works
I don’t have a strong moral view about whether physician-assisted death is inherently right or wrong. I can see why some people would want it as a last resort to end suffering, and I can also appreciate the potential risks. For me, the deciding factor is the track record of PAD laws in Oregon and other states over decades. I recognize there are limits to how well problems can be detected, but the unintended consequences and slippery slopes critics warned about have not materialized enough to sway me. Instead, the laws seem to be functioning largely as intended. On that basis, I support them.
Autonomy Has Limits
I believe strongly in patient autonomy, including the right to refuse treatment even when that leads to death. But I do not believe autonomy justifies having a physician actively help bring about one’s death. To me, there is an important moral difference between allowing a disease to take its course versus intentionally causing death, even when both follow the patient’s wishes and lead to the same outcome. That distinction marks a boundary that has long guided medical ethics. Once that boundary is crossed, I do not believe the change can be contained by safeguards or good intentions. So while I support a patient’s right to decline life-sustaining care, I oppose physician-assisted death as a step too far.
Too Many Risks
I can understand why physician-assisted death might seem compassionate in individual cases. But public policy has to be judged by its overall effects, and I think the risks here are too great. Prognoses are uncertain—some people given six months to live end up living years. Decisions that appear voluntary may be shaped by subtle pressures from family, financial strain, or a sense of being a burden, even when those pressures are not fully recognized. And the mere existence of a state-sanctioned “good death” option may create a broader social expectation around choosing it, or risk devaluing the lives of disabled and dependent people whose conditions, outside of terminal illness, resemble those of eligible patients. Much of this is difficult to measure, which should give us pause about what we might be missing. Given those uncertainties, I believe we should err on the side of protecting life rather than authorizing actions intended to end it.
Always Care, Never Kill
I oppose physician-assisted death because it is incompatible with the equal and inherent dignity of every human life. I believe dignity is intrinsic—it does not depend on autonomy, independence, or quality of life, and it does not diminish with illness, disability, or suffering. I realize this means denying physician-assisted death to some people who believe they should be entitled to it. But sometimes societies preempt individual choices for the sake of higher principles. In this case, the principle is to protect and preserve human life—and the duty of medicine is to care, not to kill.
Deciding
The debate about physician-assisted death mixes questions of mercy, personal autonomy, protecting life, social effects, and the purpose of medicine. It’s no surprise that reasonable people reach different conclusions. Our goal has been to give you the facts, arguments, and a range of viewpoints to help inform your own thinking. What you decide is up to you.
(If you are wondering about something we didn’t mention, check the Editorial Choices section below. It includes other aspects of the debate we didn’t include in the main content, with explanations why.)
Appendix: Editorial Choices
In writing this guide, there were many choices to make—for example, how to frame the issue, which factors, arguments, and viewpoints to include, and how to phrase them. For those interested, below are notable choices. You can quickly scan the topics, clicking any for details.
Naming and Framing
We recognize that perceptions can be swayed by how a topic is framed and by the terminology used. In this, as with everything else in this guide, our goal is to be fair and accurate.
Guide Name
There is no widely accepted, neutral term for this guide’s topic:
-
Supporters tend toward terms like “medical aid in dying.” Supporters usually don’t mention “suicide,” arguing it carries associations with mental illness and impulsive behavior that do not reflect end-of-life decisions under terminal illness. They also use terms like “death with dignity,” “right to die,” and “end-of-life choice,” but these are not meant to be neutral descriptions.
-
Opponents tend toward terms that include “suicide,” most prominently “physician-assisted suicide.” They argue it is appropriately descriptive, and that terms like “aid in dying” are euphemistic and could just as well refer to late-stage palliative care.
In the absence of a consensus on neutral terminology, we followed the National Academies of Sciences, Engineering, and Medicine’s choice for “physician-assisted death” as the term to use.27 However, we made clear in the subtitle and elsewhere in the guide that opponents consider it assisted suicide. We also made sure to distinguish PAD from palliative care and withdrawal of treatment in the “Facts” section.
“Physician”
We used the term “physician” rather than “doctor” because “physician” more precisely refers to clinicians licensed to practice medicine; “doctor” can also refer to people with non-medical doctoral degrees.
In some states, it is legal for an advanced registered nurse practitioner or physician assistant to evaluate and prescribe in PAD cases.28 These are licensed clinicians who can see patients and prescribe medications within their legal scope of practice. But they are not physicians: They do not complete the same level of medical training as MDs (Doctors of Medicine) and DOs (Doctors of Osteopathic Medicine).
The fact that non-physicians can sometimes evaluate patients for PAD and prescribe the lethal medication complicates the term “physician-assisted death.” We chose to still use it because of the reasons mentioned in Guide Name, and because there is no prominent alternative that captures the role of the authorized clinician. (“Authorized clinician” might be more technically accurate, but it is not a commonly used term in the PAD debate.)
“Lethal Medication”
We used the term “lethal medication” for the substances prescribed in PAD. Although U.S. PAD laws and much of the medical literature just refer to “medication,” that term has traditionally been defined in terms of curing sickness or treating symptoms, not intentionally ending a patient’s life. As a result, some opponents argue it is misleading to use the term “medication” for a substance designed to kill the patient.
We found this concern valid. As an alternative we chose “lethal medication.” The goal was to retain “medication” while making clear it is different from the traditional sense of the term. This is similar to the American Medical Association’s use of “lethal dose”29 and the American College of Physicians’ use of “lethal amount of medication.”30
Overall Framing
In the United States, the debate about physician-assisted death has a central question: Should mentally capable adults with a terminal illness be allowed to obtain medical assistance to end their own lives?
Accordingly, we chose this as the main framing for the guide. Because all existing state laws have the same general characteristics, modeled after Oregon’s first-in-the-nation law, we focused on those characteristics rather than minor variations across states.
Euthanasia
Some opponents see the American version of PAD—which limits the physician’s role to prescribing the lethal medication, not administering it—as mostly a political tactic to avoid association with euthanasia. They argue this is misleading because, in their view, the key moral aspect is the same: The physician intentionally helps the patient end their life. They note other prominent countries with PAD, like the Netherlands and Canada, consider euthanasia to be part of PAD. Thus, some opponents may conclude this guide perpetuates supporters’ agenda by accepting the non-euthanasia framing.
Our thinking: This guide is about the debate in the United States, which is about the non-euthanasia version of PAD. So the natural framing is the non-euthanasia framing. In the Slippery Slope factor, we included opponents’ concerns that current U.S. PAD laws are a wedge for later expanding to euthanasia.
Factor Choices
In debates about physician-assisted death, the arguments that most often shape people’s views tend to fall into three types of questions:
-
Moral principle: For some situations, is physician-assisted death a morally permissible—or even a morally required—response to suffering? This includes questions about whether it can be understood as an act of mercy, whether it respects or violates human dignity, and whether assisting death is meaningfully different from allowing death through the refusal of treatment.
-
Practical risks and uncertainty: Even if PAD may be justified in some cases, how confident can we be that it will be applied safely and as intended? This includes concerns about imperfect prognoses, coercion, limits of safeguards, and whether legal boundaries can remain stable over time.
-
Social meaning and institutional effects: What broader message does legalizing PAD send, and how does it reshape the roles of key institutions like medicine? This includes questions about whether PAD changes how society values certain lives, and whether it alters the ethical identity and responsibilities of physicians.
These three types of questions are reflected across the Factors to Consider. The factors provide a structure in which the different sides’ arguments can meet head-on. For a fair-minded reader, this is more helpful than simply seeing a list of each side’s talking points, which usually talk past each other.
For more on Fairmind guides’ structure and authoring principles, see Fairmind Format.
Labels for Supporters and Opponents
We used the terms “PAD supporters” and “PAD opponents” because they are descriptive and avoid advocate-defined terms like “assisted suicide” or “right to die.”
“Dignity”
In the public discourse about PAD, the word “dignity” is used in different ways, which can be confusing:
-
PAD supporters use the term “death with dignity” to mean a patient can choose the timing and manner of their death, avoiding physical or cognitive decline they would find degrading.
-
PAD opponents use the term “dignity” to refer to the inherent worth of a person, which does not depend on condition or capability. They believe this should be respected by caring for the person rather than intentionally ending their life.
In describing the debate, we used those terms as advocates use them, in their respective contexts, in distinct parts of the guide.
Advocates as Data Sources
Our preference is to cite data and analyses from neutral sources. But in some cases, we sourced data from organizations connected with advocates on one side or the other of the debate. We did so because they had the best data for the information we wanted to convey. For example:
-
Under “Facts,” there’s a map of states that do and don’t allow PAD. The data came from Death with Dignity, an advocacy organization for PAD.
-
Under “Facts,” the footnote about states that have not authorized PAD is based on data from the Charlotte Lozier Institute, a PAD opponent.
In all cases when we used data from an advocate-aligned source, we verified its accuracy and checked that it was presented fairly by comparing it with other sources.
Supreme Court Rulings
The U.S. Supreme Court has addressed physician-assisted death, most notably in Washington v. Glucksberg and Vacco v. Quill, both unanimous decisions from 1997.31 In those cases, the Court held that there is no constitutional right to physician-assisted death, leaving the issue to the states.32 Since then, PAD has developed through state legislation modeled on Oregon's 1997 statute rather than through further Supreme Court cases.
Although the 1997 cases are often mentioned in the PAD debate, we did not mention them in the main content because they did not resolve the ethical and policy debate this guide addresses. What they did establish is that PAD must be won or lost in state legislatures, not federal courts. This explains why the policy landscape today is a patchwork of state laws, and why the debate is typically framed in terms of competing policy considerations rather than constitutional rights.
Cost Savings and PAD
Opponents sometimes argue that the availability of PAD will cause insurers or health systems to push patients toward it as a way to minimize costs. They sometimes cite individual cases where an insurance company denied an expensive treatment but was willing to pay for PAD.
In researching this aspect of the debate, we found that the cases cited always had circumstances that complicated the point. For example, in 2008 Barbara Wagner was a 64-year-old woman with recurrent lung cancer. Her physician recommended a chemotherapy drug costing several thousand dollars per month. The Oregon Health Plan declined to cover the drug. In a letter, the plan stated it would cover palliative care and, if she chose it, lethal medication under Oregon’s PAD law.
In media reports, Wagner took the message to be “we’ll pay for you to die, but not pay for you to live.” The Oregon Health Services Commission responded that the letter to Wagner was poorly worded, but the coverage decision reflected Oregon’s standard Medicaid policy of prioritizing treatments. That policy does not normally cover expensive drugs with limited expected benefit. They emphasized that this was independent of PAD and noted that the letter also offered normal palliative care.33
In our view, a more relevant scenario would be if an insurer offered to pay for PAD to end a patient’s life immediately but not for palliative care that would let death occur naturally over a period of time. We found no evidence of this scenario occurring.
More generally, PAD does not appear capable of meaningfully altering the economic incentives of insurers or health-care providers. This is for a combination of reasons:
-
Few patients: In Oregon, PAD cases number in only the hundreds per year. That figure could double or triple, and it would still be a tiny number relative to all end-of-life medical cases in a year—which in turn is a tiny fraction of all Oregonians covered by insurance.
-
Limited time: Patients are only eligible for PAD when they have less than six months to live. Most take it with only days or weeks remaining in their prognosis. So there just isn’t that much time (and thus potential costs of care) saved.
-
Limited cost: In Oregon, 92% of PAD users were in hospice care, often at home.34 At that stage, expensive disease-directed treatments have typically ended, and care focuses on comfort. The remaining costs are generally lower than earlier phases of treatment.
Taken together, these are not circumstances that cause large additional expenditures for an insurer or health system.35 As a result, there is less at stake economically for insurers and healthcare providers than people might think—far less than the reputational costs that would come from having a policy channeling patients to PAD over palliative care.
For this reason, we did not include cost savings for insurers or health systems in the guide’s main content.
Financial Pressure on Patients and Families
Although PAD’s potential cost savings appear to be a nearly negligible share of insurers’ and healthcare providers’ spending, PAD could represent a meaningful cost difference versus ongoing care for an uninsured individual and family. In this view, the concern is not that institutions will steer patients toward PAD, but that some patients may steer themselves toward PAD: A terminally ill patient might weigh not only their own suffering but also the financial impact of continued care on their family—such as medical bills, caregiving burdens, or depletion of savings. Critics argue that in such situations, the option of PAD could function less as a freely chosen alternative and more as a response to economic pressure, raising questions about how voluntary such decisions truly are. Some conclude that PAD should not be legalized in a state that does not have universal healthcare insurance.36
We did not include this angle in the main content for three reasons:
-
Limited Evidence of Impact: In Oregon’s 2025 reporting about PAD patients, only 6% of cases cited “Financial implications of treatment” as a concern related to their PAD decision.37 The most commonly cited concerns related to loss of autonomy and the inability to engage in meaningful activities.
-
Applies to Other End-of-Life Decisions: Many end-of-life decisions already take place within the same financial and social constraints—for example, when a patient decides to “give up” on active interventions or to refuse treatment.
-
Prominence. It’s not a prominent argument in the discourse. If mentioned, it’s usually in passing—for example, as the observation that it is ironic for a state to allow PAD while lacking universal healthcare.
Public Opinion
PAD supporters often cite public-opinion research, which has long shown a majority of Americans supporting PAD. As of 2024, Gallup found 66% support for PAD.38 This figure comes from a question that uses the word “suicide”—relevant because Gallup’s historical data shows support runs 5–10 points higher when questions describe the intervention as “ending a patient’s life by painless means” instead of mentioning “suicide.” Nevertheless, both framings have shown majority support for decades.
We did not include a public-opinion argument in the main content for two reasons:
-
Public opinion does not determine advocates’ positions. Advocates use polling when it suits their purpose; otherwise they ignore or attack it. If the polling flipped, advocates wouldn’t change their views on PAD. They’d simply change their views on the relevance of the polling.
-
Public opinion shouldn’t be a primary reason for your own decision. The purpose of a Fairmind guide is to help you think through the substance of an issue for yourself. Letting public opinion decide for you is the opposite of that.
Also, it’s worth noting that most polls on the topic are national, whereas PAD laws are decided state by state. Each state’s public opinion will differ from national opinion, making the national results less relevant than they might initially seem.
“Fix Palliative Care First”
Opponents sometimes argue that rather than legalizing PAD, society should invest in making excellent palliative care universally available. In this view, PAD is a response to a failure of care, and the right answer is to fix the care.
We did not include this in the main content for two reasons:
-
Plausibility: The best evidence does not support the idea that palliative care, even at its most effective, can fully relieve suffering for all or even most patients. It can meaningfully reduce physical pain, but its effects on non-physical suffering are considerably less consistent.39 And there are clearly scenarios that palliative care cannot directly address, such as people losing control of bodily movement.
-
Timing: Even if it was possible to improve palliative care’s quality and availability to the point that no one would rationally choose PAD instead, achieving this would take time. Meanwhile, the question remains whether PAD should be legal now, for patients whose suffering is not being adequately addressed.
Ultimately, we saw “fix palliative care first” not as a rebuttal to the case for PAD but as a call for a separate initiative running alongside it.
Suicide Contagion
Some participants in the debate argue that legalized PAD could affect suicide rates more broadly, though they disagree which way.
Opponents sometimes argue that PAD could contribute to a “suicide contagion” effect. This draws on well-established research showing that suicide rates can be influenced by social messaging and publicized cases. In this view, normalizing PAD might affect how some at-risk individuals think about suicide more generally.
In contrast, some researchers have explored whether PAD could have a substitution or harm-reduction effect. They raise scenarios like: (1) a terminally ill patient who might otherwise die by conventional suicide instead enters the PAD process; (2) due to the process’ safeguards—medical evaluations, waiting periods, and explanations of alternatives—the patient decides against ending life through PAD or conventional suicide.
We did not include a “Suicide Contagion” standalone factor because the empirical evidence is limited and inconclusive. A small number of studies have examined whether jurisdictions with PAD laws experience changes in non-assisted suicide rates, with mixed results and significant methodological constraints. These studies do not establish a causal relationship, and they do not isolate mechanisms such as contagion or substitution.40
That said, the arguments reflect broader, well-supported ideas: that social norms can influence behavior, and that policy can shape how people respond to difficult circumstances. The Social Effects factor alludes to this.
The Hippocratic Oath and “Do No Harm”
PAD opponents often invoke the Hippocratic Oath as a reason to reject PAD. Traditionally attributed to the ancient Greek Hippocrates, the Oath is a set of ethical guidelines for physicians.41 In one passage, it states: “I will neither give a deadly drug to anybody who asked for it, nor will I make a suggestion to this effect.”42
Although the Oath is a powerful symbol of long-held wisdom, the original version is rarely used in modern medical schools.43 Oaths in use today diverge on whether to retain the prohibition against PAD; most do not include it.44
A related argument invokes the familiar phrase of medical ethics, “First, do no harm,” as an argument against PAD. The problem is, in end-of-life contexts, what constitutes harm is disputed. For some, it is a greater harm to prolong the life of a terminally ill patient who is profoundly suffering; for others, intentionally ending a life is the greater harm. Invoking “do no harm” therefore restates the underlying disagreement about PAD rather than settling it.
All that said, there is a long-standing resistance in the medical profession to PAD. We sought to reflect that in the Physicians’ Role section by quoting the American Medical Association’s opposition. In our view, that was a better way to convey the underlying concern that arguments invoking the Oath and “do no harm” are meant to express.
Advance Directives and PAD
An advance directive is a written instruction made while a person has full decision-making capacity, specifying what medical care they want—or don't want—if they later become incapacitated. Advance directives are widely used and legally recognized for decisions like refusing life-sustaining treatment. Some advocates argue that advanced directives should also be available for PAD. Ahead of time, a person could specify that PAD should be carried out if and when they reach a defined condition and are unfit mentally at that point.
In principle, this could apply to several conditions, but in practice the question concentrates on dementia, including Alzheimer’s disease. Most people with dementia lose their decision-making capacity gradually, over a period of many years. But PAD laws require the patient to have sound decision-making capacity when they request PAD, which can only be within six months or less to live. So, lacking support for advanced directives, PAD becomes impractical for most people with dementia.
This issue is real, but it is downstream from the core debate about whether PAD should be legal or not at all. As a result, we did not include it in the main content.
Post-Prescription Coercion
PAD opponents sometimes note that there is typically no requirement for a clinician or independent witness to be present when the lethal medication is self-administered. They argue this creates a potential gap at the final stage, where coercion—especially by family members or caregivers—would be hardest to detect.
We did not include this in the main text because it’s about a secondary tension in the design of PAD laws:
-
On one hand, safeguards against coercion would be tighter if clinicians were required to be present for the patient’s self-administration.
-
On the other hand, requiring the physician’s presence further implicates them in the act, deepening the role-conflict discussed in Physicians’ Role and likely shrinking the pool of physicians willing to participate.
Patient Trust
Some opponents argue that legalizing PAD undermines the trust between patient and physician. In its crudest form, patients might worry their physician will steer them toward PAD to free up resources or reduce the physician’s workload. Although it appears in the discourse, this argument is about an extremely unlikely combination of conditions: a physician acting in bad faith to encourage a patient to kill themself, a failure of safeguards like the required second opinion, and the patient (and family) going along against their interest.
A more widely applicable version of the trust concern is that the legal availability of PAD will taint the physician-patient relationship. Critics say that especially in end-of-life matters, the availability of PAD as an option invites ambiguity about the physician’s purpose and agenda, eroding trust generally.
We did not include this angle in the main content for two reasons:
-
Primary Issue Already Covered: The Physicians’ Role section covers the primary concern articulated by medical groups against PAD: that it puts physicians in a conflicted position and asks them to make judgments they’re not trained for. A potential erosion of trust is a consequence of this and tends to be raised secondarily.
-
Evidence Points the Other Way: A 2005 national survey found that only 20% of U.S. adults said they would trust their physician less if PAD were legal, with 58% disagreeing.45
Non-Legislative Pathways for Change
In the Slippery Slope section, we addressed amendments to PAD laws, such as waiting-period changes, residency rules, and types of authorized clinicians. But PAD availability and rules can also change through other means: judicial rulings, litigation seeking expansion, and clinical or administrative interpretation. For example:
-
Montana permits PAD not through a statute but through a 2009 state Supreme Court ruling that physicians can use a “consent” defense against homicide charges when assisting a terminally ill patient's suicide.46 Montana remains the only U.S. jurisdiction where PAD operates this way.
-
In Shavelson v. California Department of Health Care Services, a physician and an ALS patient sued to allow physicians to administer lethal medication for patients unable to self-administer—effectively, to expand California’s law to permit euthanasia in those cases. The court dismissed the suit in 2022, holding that such an accommodation would cross a fundamental line “from the ability to end your own life to the ability to have someone else end it for you.”47 Although the court rejected this attempt, it is nonetheless an example of how courts could be used to expand PAD.
-
Oregon’s Death with Dignity Act defines “terminal disease” as “incurable and irreversible” but does not specify whether available treatments must be tried. The Oregon Health Authority states it does not interpret the statute beyond reporting requirements.48 This has left physicians as the interpreters when unusual cases emerge. For example, a non-terminal Oregon woman with early stage dementia was able to access PAD while still being of sound mind. She voluntarily ceased to eat and drink, thereby creating what her physician judged to be a terminal condition, which resulted in a PAD prescription and her death.49
We are addressing these examples here rather than in the Slippery Slope section because, across nearly three decades of PAD in the United States, non-legislative changes have been exceptions rather than the rule. For the sake of brevity and clarity, we chose to focus the main content on the more central aspects of the debate.
Religious Arguments
Religious institutions are mostly against PAD. The Catholic Church in particular has been among the most prominent voices in opposition. That said, some smaller denominations support PAD, such as the United Church of Christ.50
If this guide was about whether you personally should undertake PAD, your personal religious beliefs would be key. But this guide is about a question of public policy: Should PAD be legal? In the U.S. legal system, laws are expected to be justifiable on non-religious grounds and to apply across people of different faiths or none.51
Also, as a practical matter, it is difficult to reason together in a pluralistic society when participants appeal to religious authority that others do not share. This is why even the Catholic Church regularly makes public policy arguments about PAD in secular terms.52
For these reasons, the guide focused on arguments framed in non-religious terms.
Further Reading
The arguments summarized in this guide were informed by a range of writings and research about physician assisted death. Beyond the citations in the footnotes, a web search will return many articles freely available online, usually taking one side or the other.
For readers who want to go deeper while keeping the fair-minded perspective, we recommend Debating Euthanasia by Emily Jackson and John Keown. Jackson is a law professor who supports PAD; Keown is an ethics and law professor who opposes it. They each articulate their side’s case on PAD and euthanasia, using language for a general audience.
Published in the United Kingdom in 2011, the book’s arguments invoke examples and experiences from countries with PAD, most prominently the Netherlands and the United States (mostly Oregon). It also often references past debates in the UK parliament, which at that point had considered and rejected PAD multiple times.
Footnotes
-
To understand the specifics of PAD in practice, see the FAQ for Oregon’s Death with Dignity Act. The Act is the model for all other U.S. state PAD laws. ↩
-
Jonathan Treem. Medical Aid in Dying: Ethical and Practical Issues. Journal of the Advanced Practitioner in Oncology 14, no. 3 (2023): 207. ↩
-
Baxter v. Montana (2009). Justia. Accessed March 26, 2026. ↩
-
Nevada and Wyoming lack a clear policy by statute or common law. PAD is generally considered to be prohibited in these states. For an annotated map of all states’ PAD statuses, see: Assisted Suicide in the States. Charlotte Lozier Institute. Accessed April 1, 2026. ↩
-
In Your State. Death With Dignity. Accessed March 26, 2026. ↩
-
Eli Y. Adashi and I. Glenn Cohen. Medical aid in dying State laws: a thirty year evolution. The Journal of the American Board of Family Medicine 38, no. 6 (2025): 977-979. ↩
-
Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 7. ↩
-
Deaths from progressive illnesses like cancer, heart disease, and neurodegenerative disease comprise a large majority of Oregon’s annual deaths. So if PAD accounts for about 1% of all deaths in Oregon, and most deaths are from progressive illnesses where PAD would be a choice, then narrowing the focus to those cases can only marginally increase PAD’s share because most of the original total already consists of such cases. ↩
-
Nikki Battiste and Carlos P. Beltran. Woman with ALS explains “Medical Aid in Dying” decision: “I don't want more time as a patient.” CBS News. January 29, 2025. ↩
-
From inception to 2025, Oregon’s PAD program saw 67% of prescribed lethal medications later ingested. Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 7. ↩
-
Palliative care is widely available in U.S. hospitals, but access is less consistent in home, outpatient, and rural settings. Studies show it can often improve quality of life by reducing pain and discomfort, although results vary depending on the patient and how care is delivered. Its effects on non-physical suffering are less consistent. (Availability of palliative care: America’s Readiness to Meet the Needs of People with Serious Illness: 2024 Serious Illness Scorecard. Center to Advance Palliative Care. August 2024. Effectiveness of palliative care: Dio Kavalieratos et al. Association Between Palliative Care and Patient and Caregiver Outcomes: A Systematic Review and Meta-analysis. Journal of the American Medical Association 316, no. 20 (2016): 2104-2114.) ↩
-
Margaret P. Battin et al. Legal physician-assisted dying in Oregon and the Netherlands: evidence concerning the impact on patients in “vulnerable” groups. Journal of Medical Ethics 33, no. 10 (2007): 591-597. Critics responded that other, harder-to-measure factors (depression, emotional state, social pressure) would better characterize the risk. (Ilora Gillian Finlay and Rob George. Legal physician-assisted suicide in Oregon and the Netherlands: evidence concerning the impact on patients in vulnerable groups—another perspective on Oregon’s data. Journal of Medical Ethics 37, no. 3 (2011): 171-174.) ↩
-
Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 9. ↩
-
For example, End Assisted Suicide is an organization working on behalf of people with disabilities to overturn states’ PAD laws. See also: Disability Groups Opposed to Assisted Suicide Laws. Not Dead Yet. Accessed May 4, 2026. ↩
-
Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 16. ↩
-
E. J. Emanuel. The history of euthanasia debates in the United States and Britain. Annals of Internal Medicine 121(10), 793-802. 1994. ↩
-
Physician Assisted Suicide. American Medical Association Code of Medical Ethics. Accessed April 6, 2026. ↩
-
Wu et al report that across 13 studies published between 2008 and 2018, live discharge rates from hospice care varied from 5% to 23%. Wu, Serena, and Deborah L. Volker. Live discharge from hospice: a systematic review. Journal of Hospice & Palliative Nursing 21, no. 6 (2019): 482-488. ↩
-
Physician Assisted Suicide. American Medical Association Code of Medical Ethics. Accessed April 6, 2026. ↩
-
Ron Acierno, Melba Hernandez-Tejada, Wendy Muzzy, and Kenneth Steve. National Elder Mistreatment Study. March 2009. ↩
-
The Oregon law grants physicians immunity from civil and criminal liability, as well as professional disciplinary action, if they participate in “good faith compliance” with the law. Supporters argue that immunity is necessary because, without it, no doctor would risk their license or a potential homicide charge to fulfill a patient’s legal request. They note that immunity does not exist for bad-faith actions such as willful negligence, forging a request for PAD, or ignoring evidence of undue influence. ↩
-
Physician-assisted suicide: A family struggles with the question of whether mom is capable of choosing to die. The Oregonian. October 17, 1999. ↩
-
In 2025, the number of cases referred for psychiatric evaluation was less than 1%. Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 15. ↩
-
Hibah Khaja. Medical Aid in Dying: Navigating Evolving Laws, Institutional Policies, and Professional Ethical Guidelines. Clinical Advisor. September 17, 2025. ↩
-
New medical assistance in dying legislation becomes law. Department of Justice Canada. March 17, 2021. ↩
-
States Abandon Initial “Safeguards” to Expand Assisted Suicide Laws. Patients Rights Action Fund. 2024. ↩
-
National Academies of Sciences, Engineering, and Medicine. 2018. Physician-Assisted Death: Scanning the Landscape: Proceedings of a Workshop. Washington, DC: The National Academies Press. ↩
-
For example, New Mexico: Elizabeth Whitefield End-of-Life Options Act. NMHealth. Accessed May 4, 2026. ↩
-
Physician Assisted Suicide. American Medical Association Code of Medical Ethics. Accessed May 16, 2026. ↩
-
Policy Compendium, Winter 2021. The American College of Physicians. February 10, 2021. Page 53. ↩
-
Washington v. Glucksberg (1997). Justia. Accessed April 13, 2026. Vacco v. Quill (1997). Justia. Accessed April 13, 2026. ↩
-
Physician Assisted-Death and Substantive Due Process. Constitution Annotated. Accessed April 6, 2026. ↩
-
Tim Christie. A Gift of Treatment. The Register-Guard. June 3, 2008. ↩
-
Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 9. ↩
-
Ezekiel J. Emanuel and Margaret P. Battin. What are the potential cost savings from legalizing physician-assisted suicide? New England Journal of Medicine 339, no. 3 (1998): 167-172. ↩
-
Robert P. Jones interviewed by David Masci. A Progressive Argument Against the Legalization of Physician-Assisted Suicide. Pew Research Center. October 3, 2007. ↩
-
Oregon Death with Dignity Act: 2025 Data Summary. Oregon Health Authority. April 1, 2026. Page 16. ↩
-
Rachel Yi. Most Americans Favor Legal Euthanasia. Gallup. August 8, 2024. ↩
-
Dio Kavalieratos et al. Association Between Palliative Care and Patient and Caregiver Outcomes: A Systematic Review and Meta-analysis. Journal of the American Medical Association 316, no. 20 (2016): 2104-2114. ↩
-
Anne M. Doherty, Caitlyn J. Axe, and David A. Jones. Investigating the relationship between euthanasia and/or assisted suicide and rates of non-assisted suicide: systematic review. BJPsych Open 8, no. 4 (2022): e108. ↩
-
Laura McPherson. The History of the Hippocratic Oath. Northeastern University. June 3, 2015. ↩
-
Hippocratic Oath (Classical Version). Dalhousie University Libraries. Updated December 18, 2025. ↩
-
Shernaz S. Dossabhoy, Jessica Feng, and Manisha S. Desai. The use and relevance of the Hippocratic Oath in 2015—a survey of US medical schools. Journal of Anesthesia History 4, no. 2 (2018): 139-146. ↩
-
Orr et al, report that as of a 1993 survey of North American medical schools, 14% used an oath that included a prohibition on PAD (“euthanasia” in the survey). Robert D. Orr, Norman Pang, Edmund D. Pellegrino, and Mark Siegler. Use of the Hippocratic Oath: A Review of Twentieth Century Practice and a Content Analysis of Oaths Administered in Medical Schools in the U.S. and Canada in 1993. The Journal of Clinical Ethics 8, no. 4 (Winter 1997): 377-88. ↩
-
M. Hall, F. Trachtenberg, and E. Dugan. The impact on patient trust of legalising physician aid in dying. Journal of Medical Ethics 31, no. 12 (2005): 693-697. ↩
-
Baxter v. Montana (2009). Justia. Accessed March 26, 2026. ↩
-
Shavelson v. California Department of Health Care Services. GovInfo. June 22, 2022. ↩
-
Public Health’s Role: Oregon’s Death with Dignity Act. Oregon Health Authority. Accessed May 4, 2026. ↩
-
Pope, T.M. & Brodoff, L.S. Medical aid in dying to avoid late-stage dementia. Journal of the American Geriatrics Society 72, no. 4 (2024): 1216-1222. ↩
-
Religious Groups’ Views on End-of-Life Issues. Pew Research Center. November 21, 2013. ↩
-
For a historical perspective on U.S. law’s non-religious purpose and justification, see the analysis of Lemon v. Kurtzman in the U.S. Library of Congress’ Constitution Annotated. ↩
-
See Top Reasons to Oppose Assisted Suicide by the U.S. Conference of Catholic Bishops. It is four pages of argumentation against PAD, with no religious claims. ↩
Thank you for reading! How likely are you to recommend this guide to a friend interested in the topic?
0 = Not at all likely, 10 = Extremely likely